
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
肺癌放射性肺炎危险因素的Meta分析
[段晨阳a , 刘梦颖a , 吴剑a , 张杰a , 张吉强b  ]
]
]
|
|


作者简介:段晨阳与刘梦颖并列第一作者。段晨阳(1991-),男,石家庄人,在读硕士研究生,主要研究方向为肿瘤医学研究。刘梦颖(1992-),女,河北沧州人,在读硕士研究生,主要研究方向为肿瘤医学研究。
目的 探讨影响放射性肺炎发生的因素,为更好地指导临床治疗、减少放射性肺炎的发生提供依据。方法计算机检索PubMed数据库、EMBASE数据库、Cochrane协作网和CNKI数据库,并辅以手工检索等方法,应用RevMan 5.1软件对截止2012年2月发表的预测肺癌放疗后发生放射性肺炎的文献数据进行Meta分析。结果共纳入文献75篇。暴露因素包括患者自身因素(性别、年龄、慢性肺疾病、肺功能、合并糖尿病)、肿瘤部位、治疗方案(放疗前有无手术、是否行联合放化疗及使用放疗增敏剂阿米福汀)。Meta分析结果显示其比值比及其95%可信区间分别为:性别0.97[0.82,1.15],年龄0.90[0.63,1.28],合并慢性肺疾病2.18[1.59,3.00],放疗前肺功能0.27[0.11,0.65],合并糖尿病2.46[1.33,4.58],左下肺部肿瘤0.71[0.57,0.90],放疗前肺部手术0.92[0.67,1.25],放化疗联合1.41[1.17,1.71],使用放疗增敏剂阿米福汀2.38[1.79,3.16]。结论影响放射性肺炎发生的因素有合并慢性肺疾病、放疗前肺功能、糖尿病、左下肺部肿瘤、放化疗联合以及使用放疗增敏剂阿米福汀。本项研究的结果认为肺功能较好且无慢性肺疾病和糖尿病等合并症的上肺肺癌患者,在单纯放疗的基础上加用放疗增敏剂阿米福汀,可以降低患者的放射性肺炎发生率。
Objective To study the risk factors of radiation pneumonitis in order to find prognostic parameters and provide reference standard for the best clinical treatment plan.Methods The database of PubMed, EMBASE, Cochrane Library and CNKI were searched from the date of their establishments to Februɑry 2012, and other supplied sources were also retrieved. Meta-analysis on literatures predicting radiation pneumonitis after radiotherapy were conducted by using RevMan 5.1 software.Results A total of 75 studies were included. The exposure factors included the patient's own factors (sex, age, chronic lung disease, pulmonary function, diabetes), tumor site, therapeutic schedule (operation before radiotherapy, combined radiochemotherapy, using radiotherapy sensitization agent Amifostine). Meta-analysis results showed that the OR and 95%CI of each factors were: 0.97[0.82,1.15], 0.90[0.63,1.28], 2.18[1.59,3.00], 0.27[0.11,0.65], 2.46[1.33,4.58], 0.71[0.57,0.90], 0.92[0.67,1.25], 1.41[1.17,1.71], 2.38[1.79,3.16], respectively.Conclusions The risk factors of radiation pneumonitis are chronic lung disease, pulmonary function, diabetes, tumor located in left lower lung, combined radiochemotherapy and using radiotherapy sensitization agent Amifostine. The study results indicate that upper lung cancer patients with good pulmonary function and without comorbidity such as diabetes or chronic pulmonary disease have less chance getting radiation pneumonitis based on the simple radiotherapy added with Amifostine—a radiotherapy sensitizer.
肺癌是世界上死亡率最高的恶性肿瘤,大约2/3的肺癌患者需要接受放射治疗。随着放射治疗技术的飞速发展,伴随的毒副作用,包括放射性肺损伤(radiation lung injury)也成为一个日益突出的问题。据国外资料统计,急性放射性肺损伤的发生率为5%~36%[ 1, 2],由此造成的呼吸衰竭是放射性肺损伤的主要致死原因之一。放射性肺损伤分为早期急性放射性肺炎(radiation pneumonitis, RP)和晚期放射性肺纤维化(radiation pulmonary fiberosis, RPF),二者是连续的过程,目前临床上尚没有令人满意的治疗措施和有效的预测手段,而放射性肺炎一旦发生,将直接影响到患者的治疗效果和生存质量。因此,对放射性肺损伤的预测已成为医学领域中的一项重要课题。本研究对截止2012年2月发表的预测肺癌放疗后发生放射性肺炎的文献进行Meta分析,以期得到影响放射性肺炎发生的因素,为更好地指导临床治疗、减少放射性肺炎的发生提供依据。
以“肺癌(lung cancer)”、“ 放射性肺炎(radiation pneumonitis)”、“ 放射性肺损伤(radiation lung injury)”为关键词在PubMed数据库、EMBASE数据库、Cochrane协作网以及CNKI数据库中进行检索。所有检索均截止至2012年2月,手工检索相关期刊,必要时向有关专家索要相关研究资料。
纳入标准:①研究对象为经细胞学或病理学确诊为原发性肺癌的首次行肺部放射治疗的患者;②文献中记录了各暴露因素发生放射性肺炎及非放射性肺炎的例数、百分比或均数±标准差(mean±SD);③对同一研究组观察不同年限的结果,仅取观察年限最长、最新发表的研究。
排除标准:①无法获得全文的会议摘要;②入组患者同时行胸部其他部位的放疗,或曾在治疗前1年内行胸部放疗;③研究结果为放射性肺纤维化;④评分差的文献;⑤重复发表的文献。
由两人各自独立地完成对入选研究进行资料摘录。将发生放射性肺炎的患者视为放射性肺炎组,未发生放射性肺炎的患者视为非放射性肺炎组。
病例对照研究及队列研究使用Newcastle-Ottawa评分标准[ 3],根据病例的选择、设计和分析的可比性、暴露或结局的确定及评估等三方面进行质量评估;随机对照研究采用CONSORT 2010声明进行评分,共计25项,分别从文章题目及摘要、引言、方法(主要包括试验设计、干预措施、结局指标、随机方法、盲法、统计分析等)、结果(主要包括受试者流程、基线资料、结局及危害等)、讨论(局限性、可推广性)及其他信息进行评价[ 4]。
应用Cochrane协作网提供的RevMan 5.1软件。采用Q检验明确有无异质性。经Q检验若无明显统计学差异( P>0.10,或 P≤0.10且 I2≤50%),选用固定效应模型进行分析;若有统计学差异( P≤0.10且 I2>50%),则选用随机效应模型。整合结果以 P≤0.05为差异有统计学意义。敏感性分析用于判断结果的稳定性和强度。主要包括:改变纳入标准、研究质量的高低、统计模型和效应量,观察两种模型的效应值整合结果和异质性有无变化。发表偏倚的识别常采用绘制漏斗图,漏斗图对称则说明发表偏倚得到有效控制。
按纳入标准通过浏览目录和摘要初步检索出文献75篇[ 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42, 43, 44, 45, 46, 47, 48, 49, 50, 51, 52, 53, 54, 55, 56, 57, 58, 59, 60, 61, 62, 63, 64, 65, 66, 67, 68, 69, 70, 71, 72, 73, 74, 75, 76, 77, 78, 79],其中Nakayama、Vujaskovic等[ 78, 79]的研究因病例数少,根据Newcastle-Ottawa评分较低而排除。纳入的文献中有6篇[ 63, 83, 84, 85, 86, 87]对放射性肺炎的发生率与使用放疗增敏剂阿米福汀的关系进行分析,均为随机对照试验,其中1篇文献有两组数据[ 73]。其余68篇文献均为病例对照研究。纳入的研究均描述了纳入及排除标准,放射性肺炎的诊断标准、随访时间及失访率等内容。暴露因素包括患者自身因素(性别、年龄、慢性肺疾病、肺功能、合并糖尿病),肿瘤部位,治疗方案(放疗前有无手术、是否行联合放化疗及使用放疗增敏剂阿米福汀)等。
对入组文献进行全文阅读,提取了以下内容:①文献一般资料(包括作者姓名、发表年份、作者单位等信息);②研究对象资料(研究例数、是否为原发性肺癌或与其他类型肿瘤同时分析等);③观察终点(放射性肺炎的诊断及分级、放射性肺炎发生例数等);④各个暴露因素下放射性肺炎组与非放射性肺炎组的数值或比例;⑤对于等级资料,提取上述参数不同等级情况下两组的病例数或百分比;对于连续性资料,提取两组的例数及上述参数的mean±SD。
2.3统计学结果2.3.1患者自身因素
2.3.1.1性别18篇文献2 178例样本纳入分析,Q检验无异质性,采用固定效应模型计算比值比(odds ratio,OR)及95%可信区间(confidence interval,CI)为0.97[0.82,1.15], P=0.73,提示差异无统计学意义。
2.3.1.2年龄10篇文献880例以≤60岁vs. >60岁分析,10篇1 396例以≤70岁vs. >70岁分析, 6篇621例分析年龄mean±SD与放射性肺炎发生率的关系。效应值合并后均无异质性,采用固定效应模型得OR及95%CI值分别为0.90[0.63,1.28]、1.13[0.84,1.52]及-0.01[-1.98,1.96], P分别为0.56、0.34及1.00,均与放射性肺炎的发生无相关性。
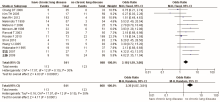
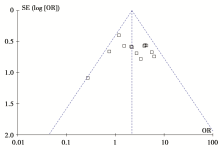
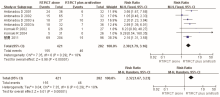
2.3.1.3合并慢性肺疾病13篇共1 409例进行分析,无异质性,固定效应模型得OR及95%CI值为2.18[1.59,3.00], P<0.000 01,提示合并慢性肺疾病的患者容易发生放射性肺炎;调整模型后OR及95%CI值为2.35[1.57,3.51], P<0.000 1,两种模型结果一致,结果可信,见 图1和 图2。
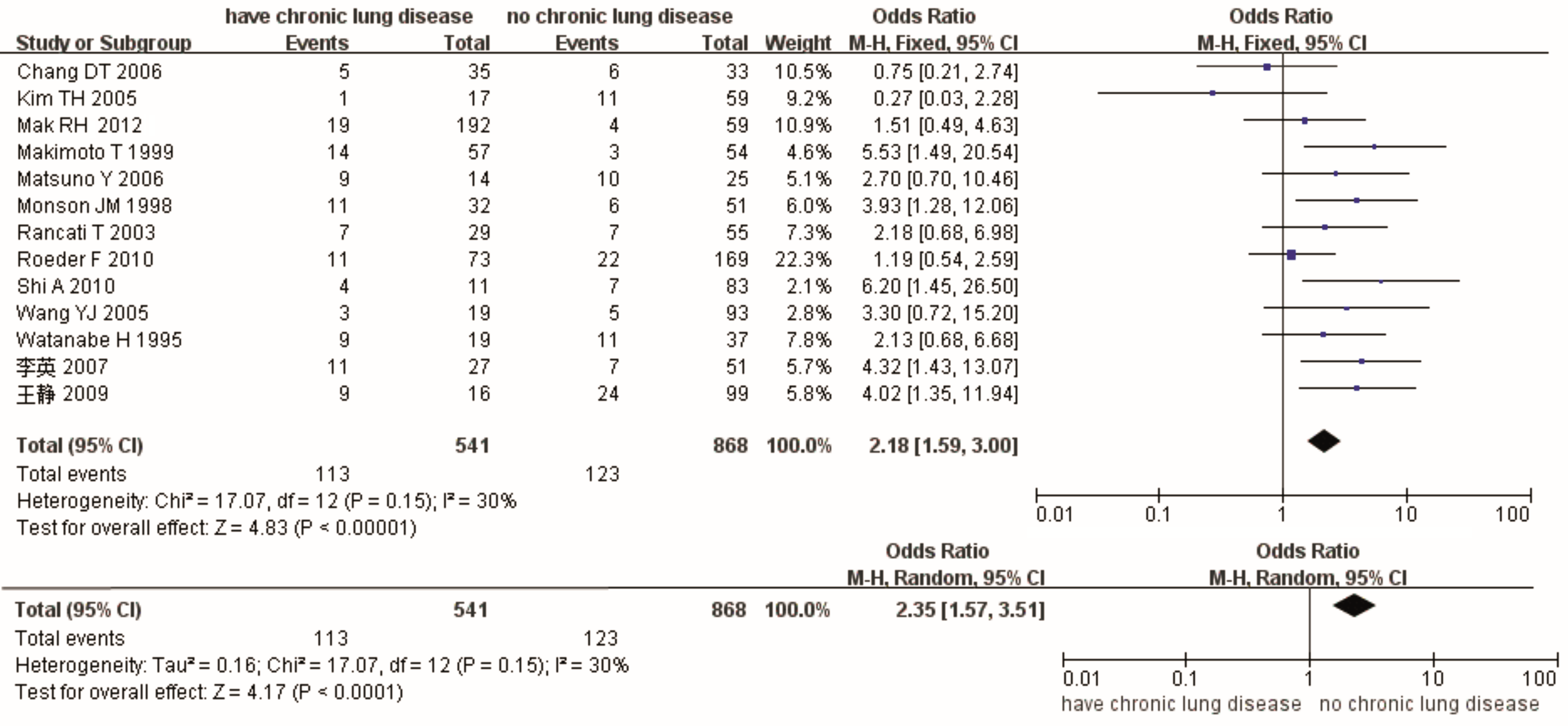 | 图1 有无慢性肺疾病与RP的效应值比较及敏感性分析图 |
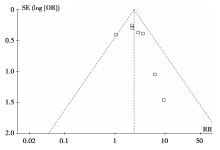
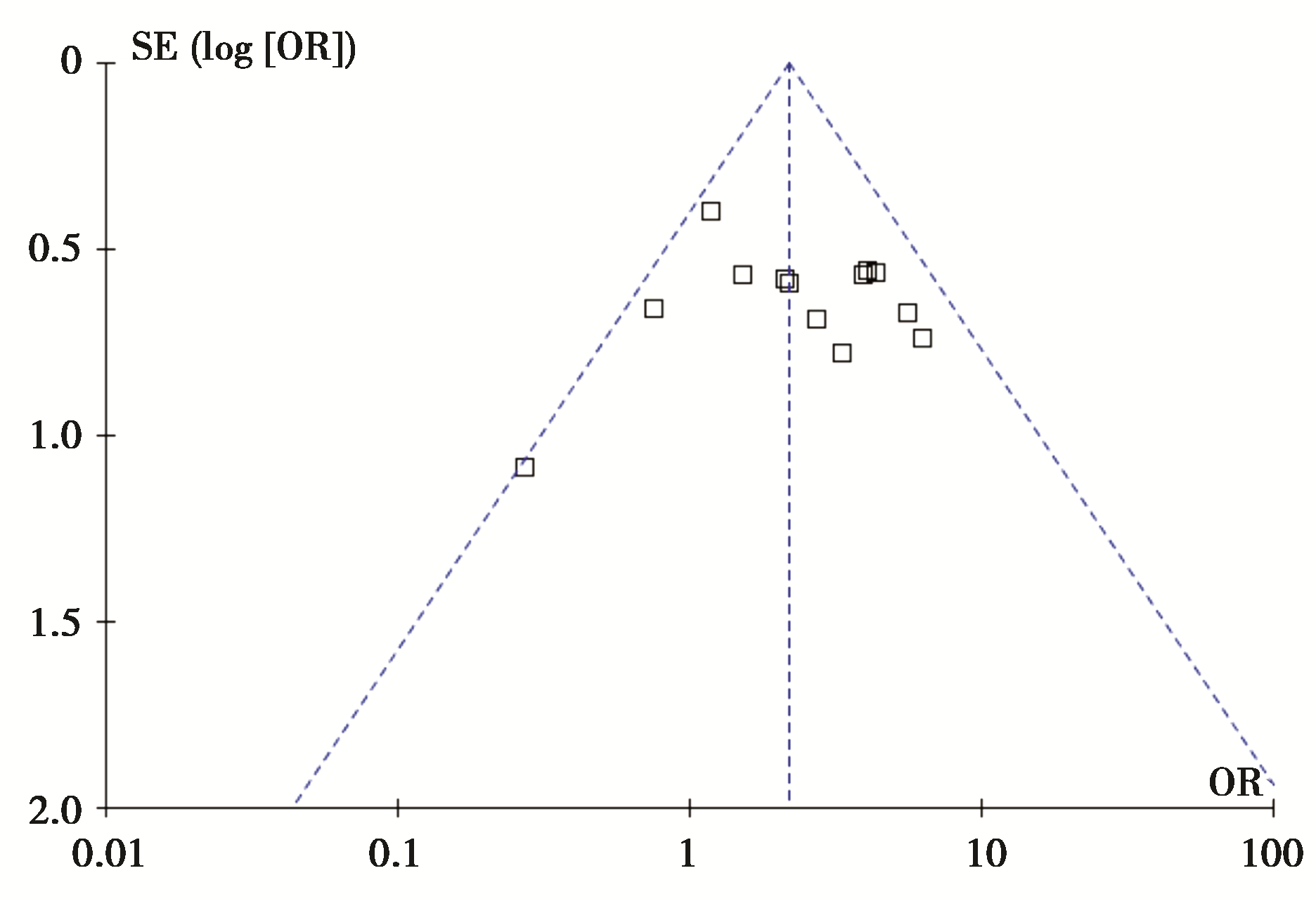 | 图2 有无慢性肺疾病与RP的倒漏斗图 |
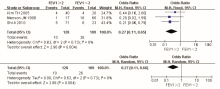
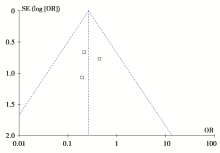
2.3.1.4放疗前肺功能放疗前1秒用力呼气量(forced expiratory volume in 1s, FEV1)≥2L vs. <2L与放射性肺炎的分析,无异质性,固定效应模型得OR及95%CI为0.27[0.11,0.65], P=0.004,提示放疗前FEV1<2L的患者发生放射性肺炎的概率较高。调整模型后,OR及95%CI分别为0.27[0.11,0.66], P=0.004,两种模型结果一致,结果可信,见 图3。但倒漏斗图未完全显示,考虑存在发表偏倚,见 图4。
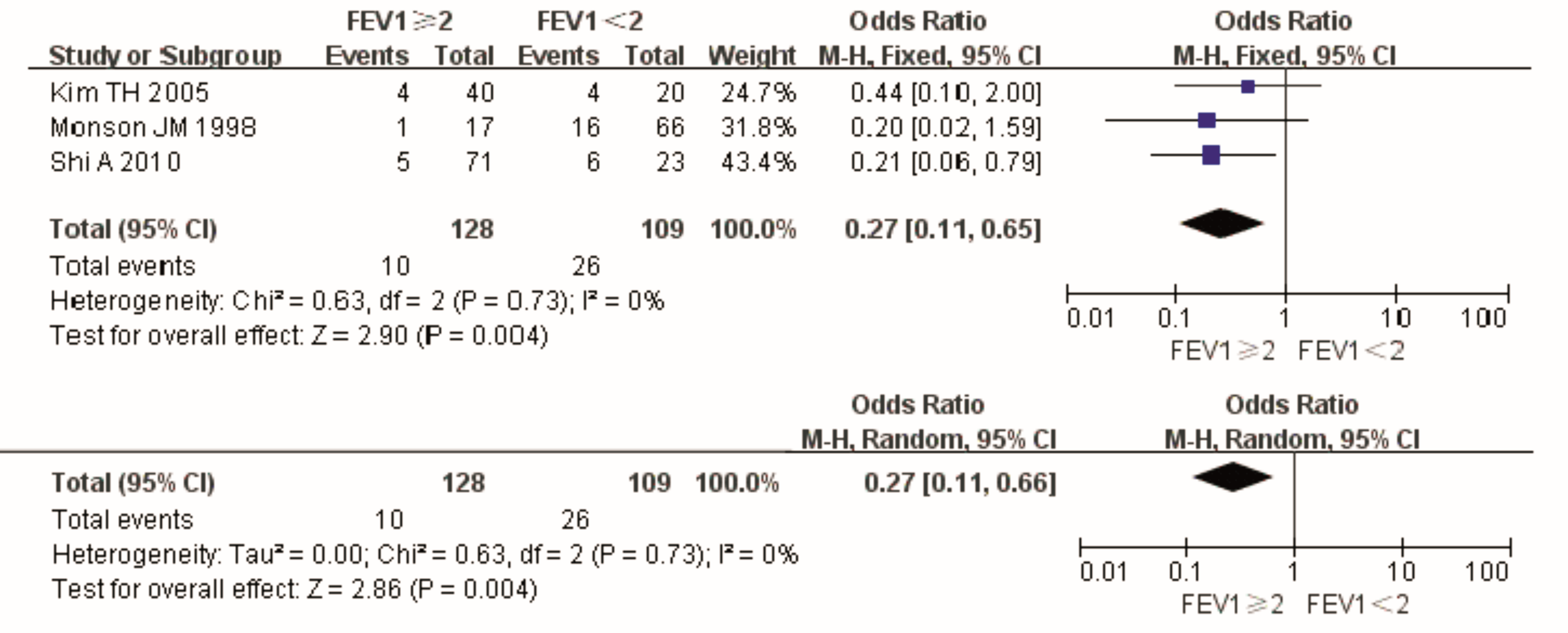 | 图3 放疗前FEV1≥2或<2L与RP的效应值比较及敏感性分析图 |
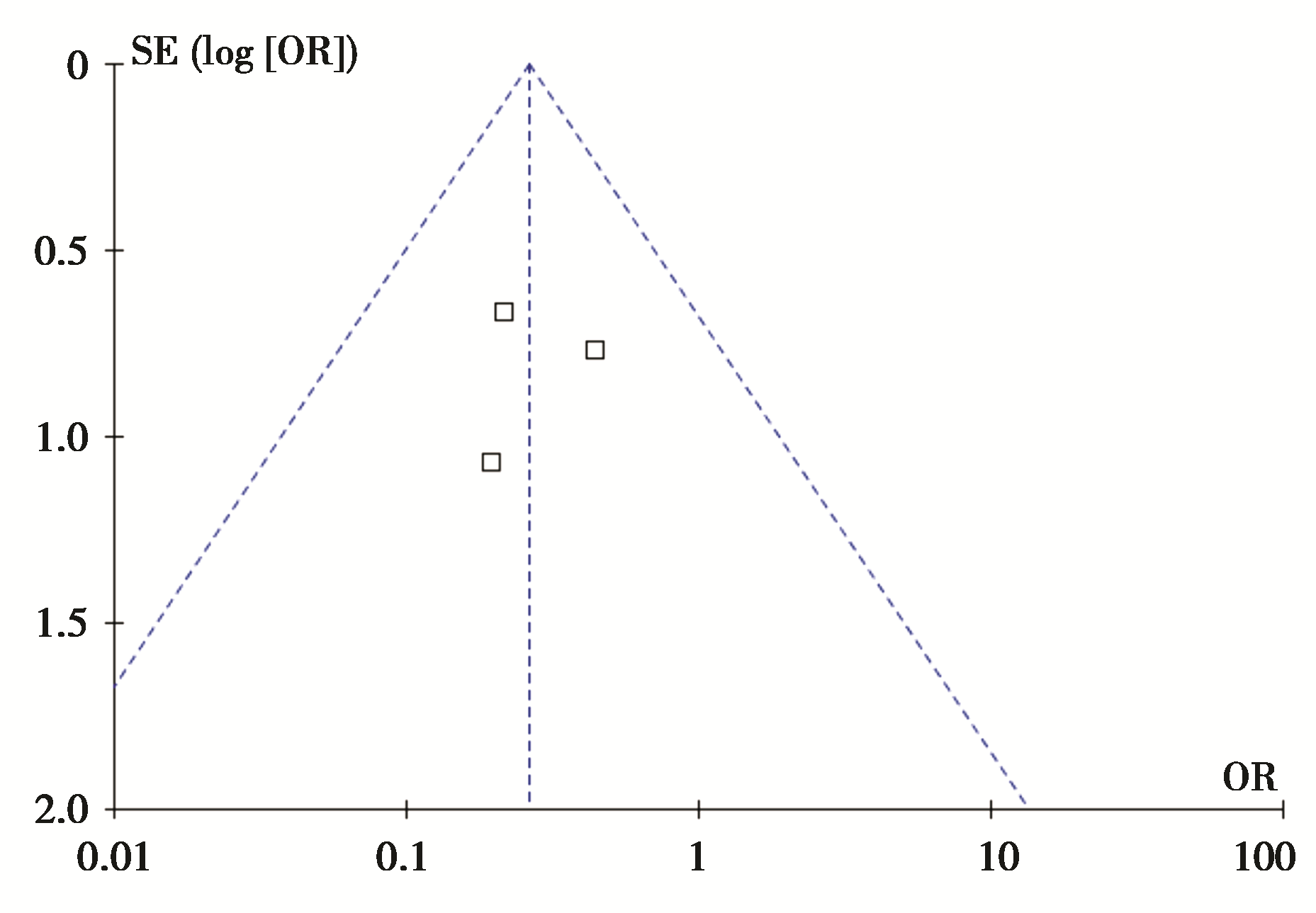 | 图4 放疗前FEV1≥2或<2L与RP的倒漏斗图 |
2.3.1.5糖尿病3篇365例样本量对此进行分析,无异质性,OR及95%CI为2.46 [1.33, 4.58], P=0.004,表明合并糖尿病的患者易于发生放射性肺炎。调整模型后,OR及95%CI为2.46[1.32,4.60], P=0.005,两模型结果一致,敏感性较低,稳定性结果,结果可信,见 图5和 图6。
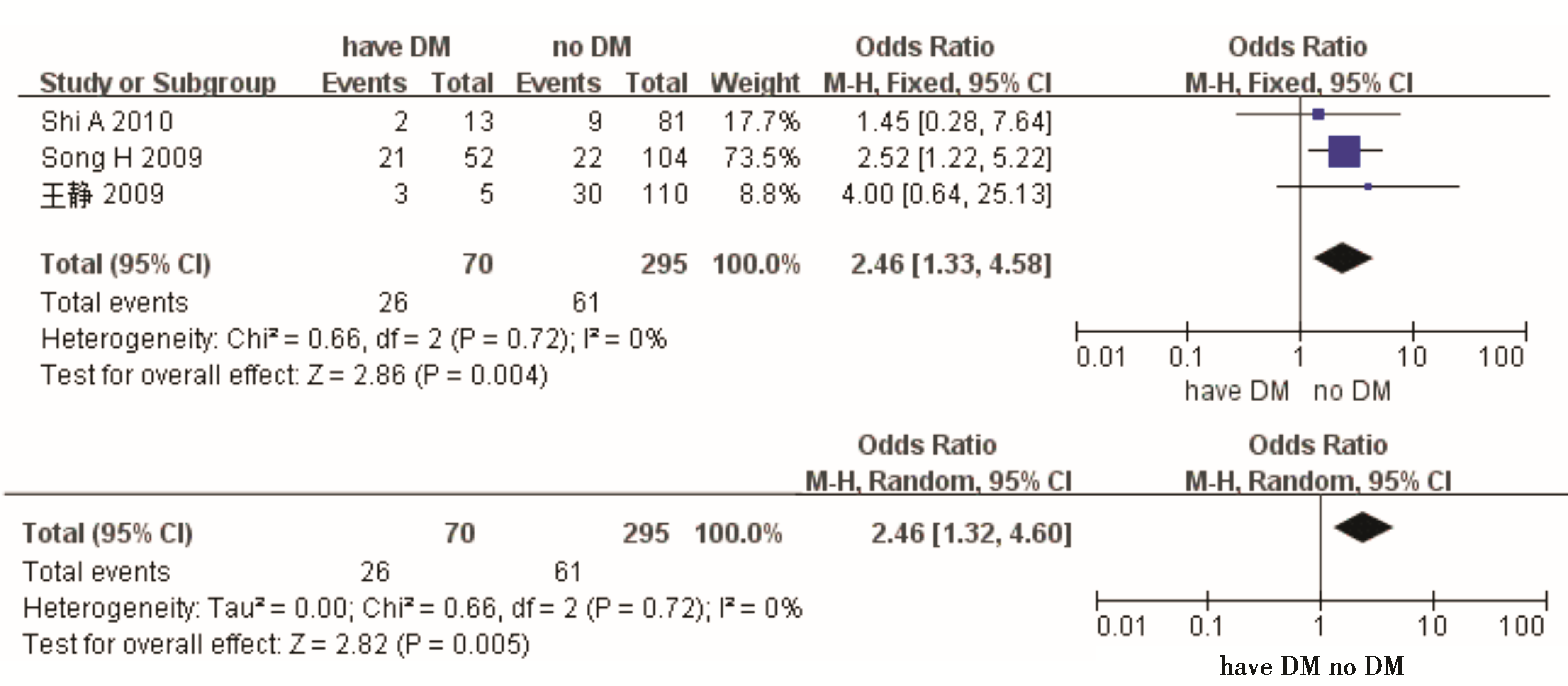 | 图5 有无糖尿病与RP的效应值比较及敏感性分析图 |
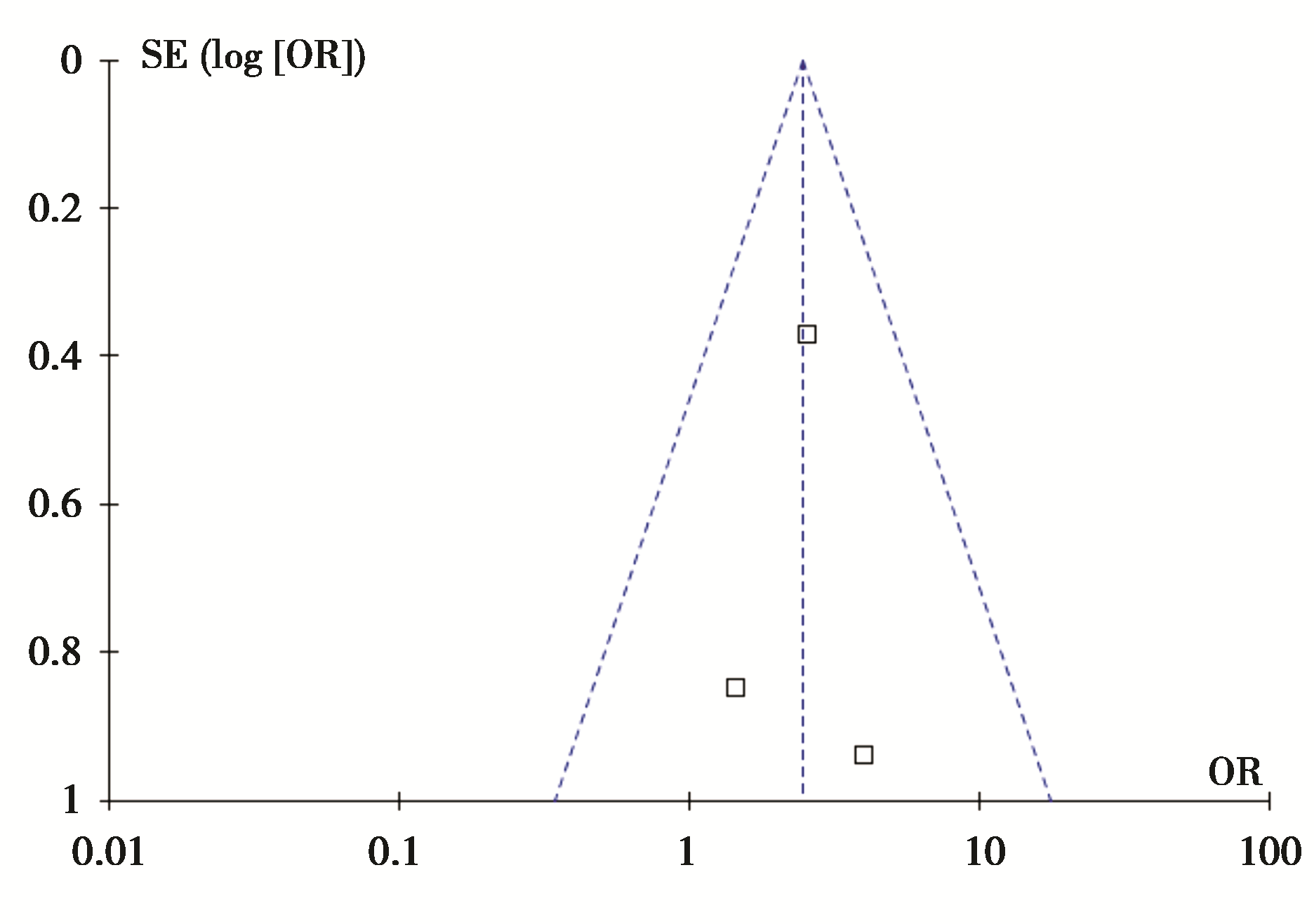 | 图6 有无糖尿病与RP的倒漏斗图 |
2.3.2肿瘤部位13篇2 211例、9篇1 880例及3篇381例患者分别对上肺vs. 中下肺、右肺vs. 左肺、中央型vs. 周围型进行分析,合并后均无异质性,OR及95%CI分别为0.71[0.57,0.90]、1.18[0.91,1.52]、1.33[0.76,2.35], P为0.005、0.21、0.32,提示肿瘤位于左下肺放疗后易于发生放射性肺炎。调整为随机效应模型,OR及95%CI分别为0.74[0.56,0.99]、 1.17[0.90,1.52]、 1.32[0.74,2.33], P分别为0.04、0.23、0.34,两种结果一致,敏感性较低,稳定性较高,结果可信。
2.3.3治疗因素
2.3.3.1放疗前肺部手术Q检验无异质性,OR及95%CI值为0.92[0.67,1.25], P=0.59,提示无相关性;随机效应模型得OR及95%CI值为0.86[0.53,1.41], P=0.56,两组结果一致,稳定性高,结果可信。
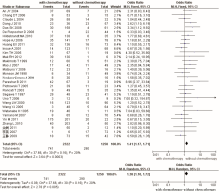
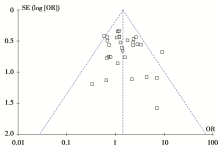
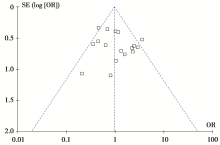
2.3.3.2放化疗联合分别有31篇3 572例和18篇1 760例样本量进行放化疗联合vs.单独放疗、序贯vs. 同步放化疗的分析,均无异质性,OR及95%CI分别为1.41[1.17,1.71]及0.97 [0.76,1.25], P分别为0.000 3及0.83,说明放化疗联合的患者易于发生放射性肺炎;随机效应模型下OR及95%CI分别为1.38[1.10,1.72]及1.02[0.71,1.47], P分别为0.005及0.90,两组结果差别不大,稳定性较高,结果可信,见 图7~ 图10。
 | 图7 放化疗联合或单独放疗与RP的效应值比较及敏感性分析图 |
| 图8 序贯或同步放化疗与RP的效应值比较及敏感性分析图 |
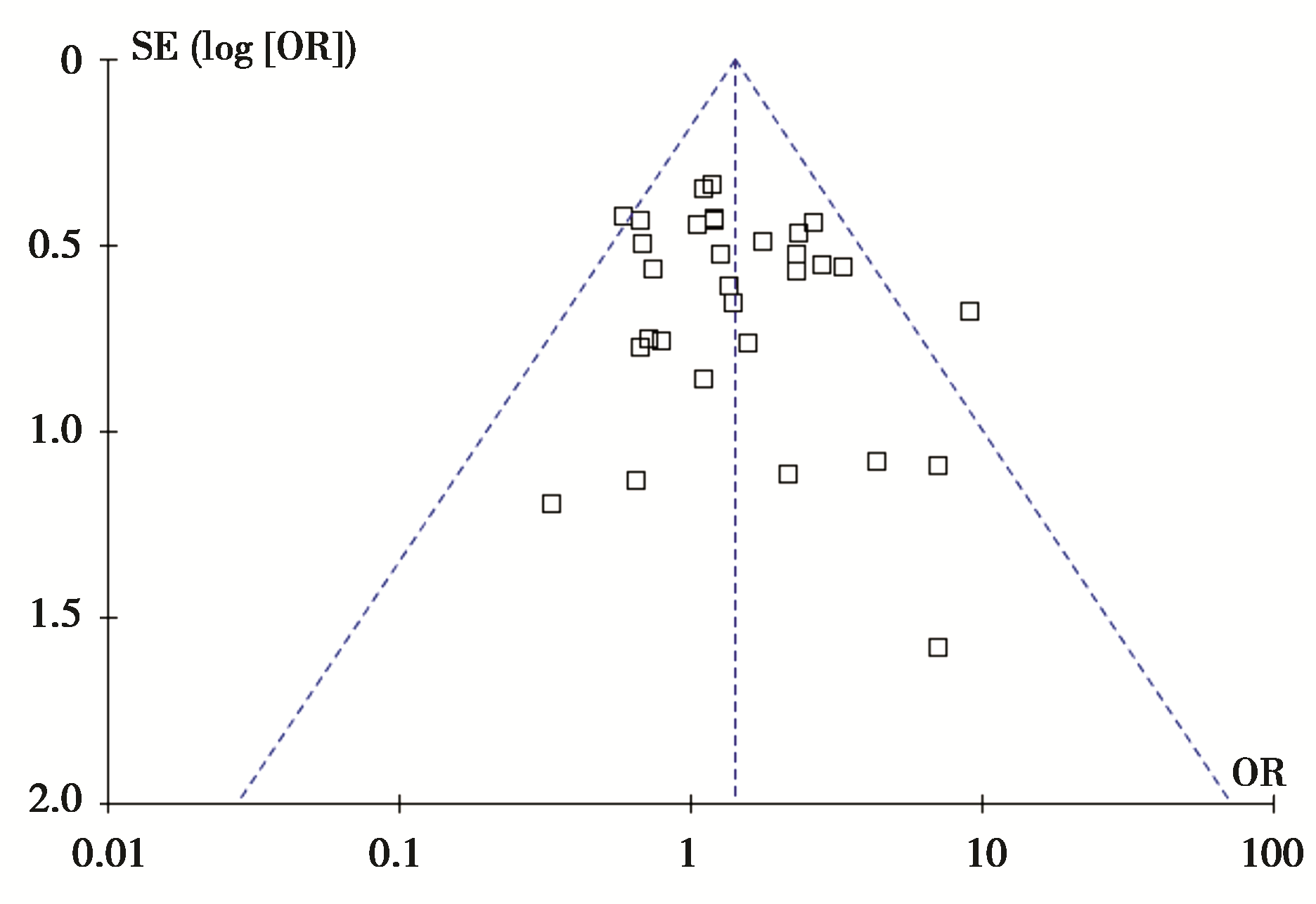 | 图9 放化疗联合或单独放疗与RP的倒漏斗图 |
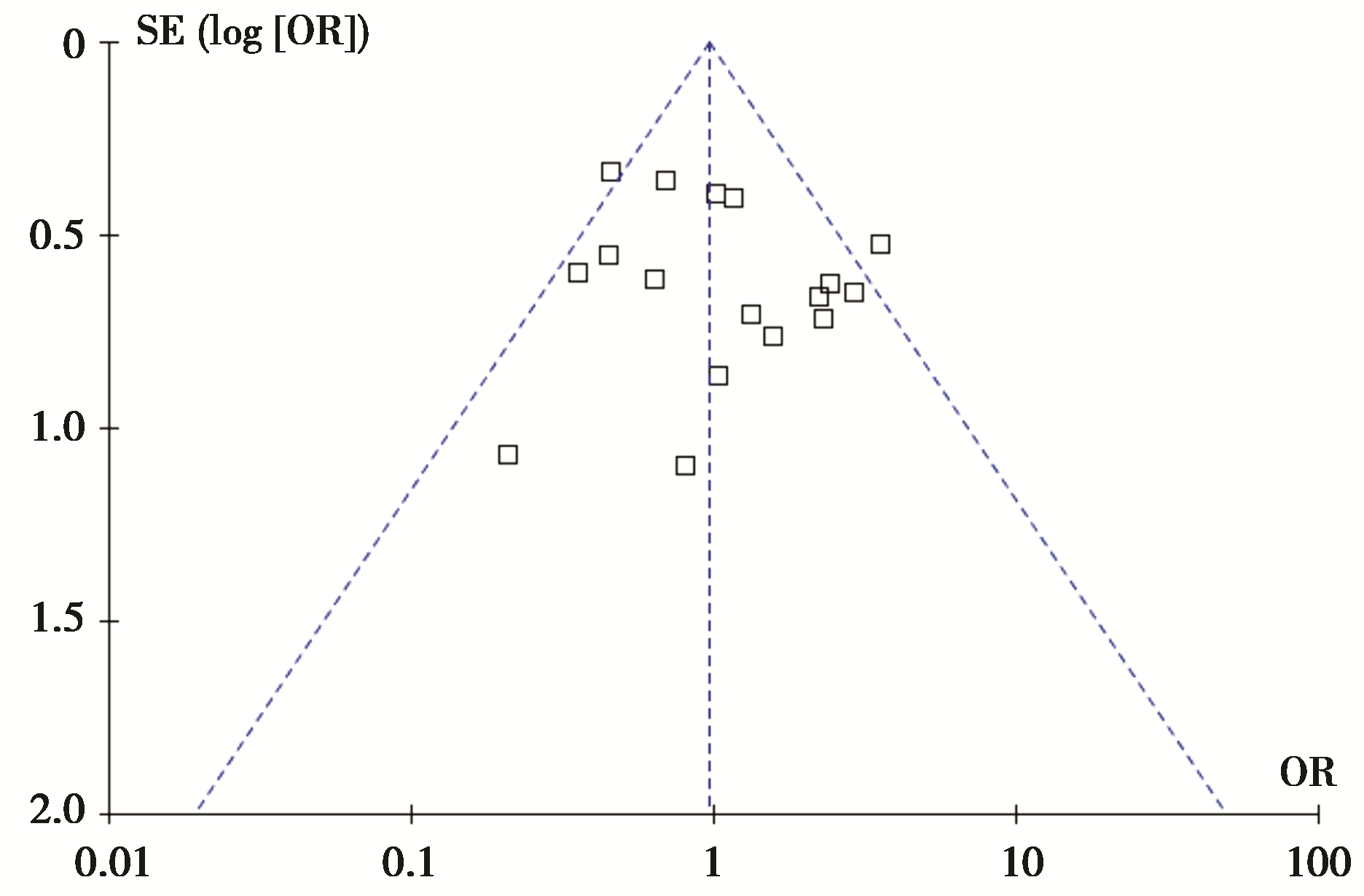 | 图10 序贯或同步放化疗与RP的倒漏斗图 |
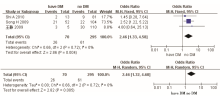
2.3.3.3放疗增敏剂阿米福汀7篇703例样本量进行分析,Q检验无异质性,由于纳入文献为随机对照试验,选用相对危险度(relative risk,RR)作为效应值,固定效应模型得RR及95%CI为2.38[1.79,3.16], P<0.000 01,说明该因素与放射性肺炎的发生有关;调整模型后,RR及95%CI为2.32[1.67,3.23], P<0.000 01,两种结果一致,结果可信,见 图11和 图12。
 | 图11 单独放化疗或联合阿米福汀与RP的效应值比较及敏感性分析图 |
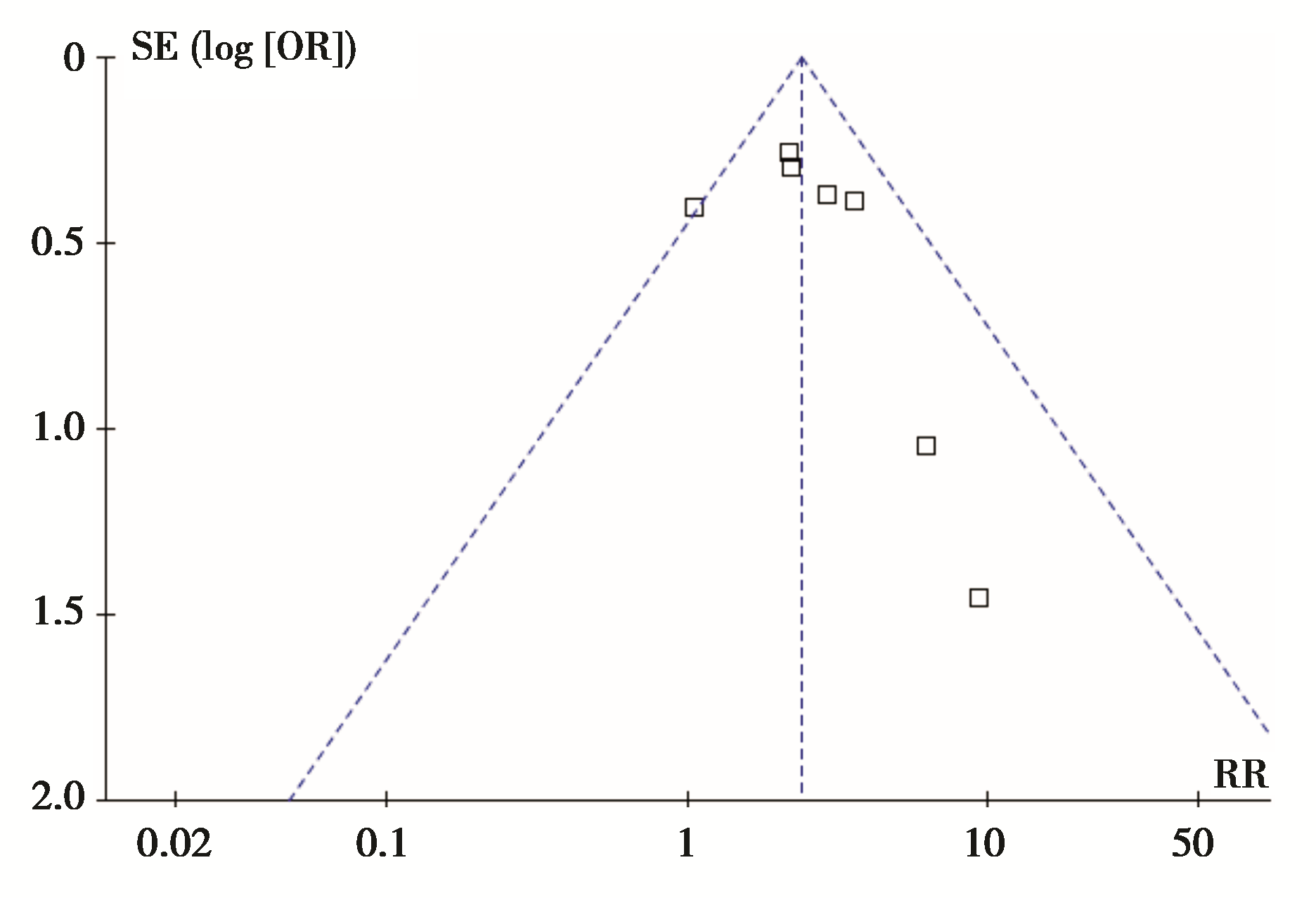 | 图12 单独放化疗或联合阿米福汀与RP的倒漏斗图 |
放射性肺炎是胸部放疗剂量的主要限制性因素,同时也是影响患者放疗后生存质量的最常见因素之一,使得最大程度提高靶区剂量且尽可能减少放射性肺炎的发生成为肺癌治疗策略必须考虑的因素,也是待解决的热点问题之一。
目前部分研究认为,临床因素方面,性别、年龄身体状况及肺功能、肿瘤及治疗因素与放射性肺炎有关。Dang 等[ 11]的研究认为,男性患者放疗后容易发生放射性肺炎,但较多研究认为女性容易发生[ 5, 28],考虑女性肺体积相对较小,同样的照射野更容易发生放射性肺炎。目前的研究普遍认为放化疗联合治疗[ 10, 11, 26, 72]、合并慢性肺疾病[ 7, 16, 26]和放疗前肺功能较差[ 7, 16, 28]的患者存在化疗对肺组织的毒副作用、有效肺体积较小及低氧等引起放射性肺损伤的病理生理过程,因此容易发生放射性肺炎。对于与吸烟的关系,尚未得到统一的结论。Vogelius等[ 80]的系统评价显示老年患者、肿瘤位于中下肺、存在合并症等是放射性肺炎的危险因素,而当前吸烟和有吸烟史是保护因素,考虑可能是吸烟所致的低氧和免疫抑制作用使吸烟患者的肺的耐受性增加。
本文的结果均经过异质性分析及敏感性检验,结果可信。本文还利用敏感性分析评估了发表偏倚对最后结果的可能影响。基于本项研究的结果,我们认为肺功能较好的且无慢性肺疾病和糖尿病等合并症的上肺肺癌患者,在单纯放疗的基础上加用放疗增敏剂阿米福汀,可以降低患者的放射性肺炎发生率。
| [1] |
|
| [2] |
|
| [3] |
|
| [4] |
|
| [5] |
|
| [6] |
|
| [7] |
|
| [8] |
|
| [9] |
|
| [10] |
|
| [11] |
|
| [12] |
|
| [13] |
|
| [14] |
|
| [15] |
|
| [16] |
|
| [17] |
|
| [18] |
|
| [19] |
|
| [20] |
|
| [21] |
|
| [22] |
|
| [23] |
|
| [24] |
|
| [25] |
|
| [26] |
|
| [27] |
|
| [28] |
|
| [29] |
|
| [30] |
|
| [31] |
|
| [32] |
|
| [33] |
|
| [34] |
|
| [35] |
|
| [36] |
|
| [37] |
|
| [38] |
|
| [39] |
|
| [40] |
|
| [41] |
|
| [42] |
|
| [43] |
|
| [44] |
|
| [45] |
|
| [46] |
|
| [47] |
|
| [48] |
|
| [49] |
|
| [50] |
|
| [51] |
|
| [52] |
|
| [53] |
|
| [54] |
|
| [55] |
|
| [56] |
|
| [57] |
|
| [58] |
|
| [59] |
|
| [60] |
|
| [61] |
|
| [62] |
|
| [63] |
|
| [64] |
|
| [65] |
|
| [66] |
|
| [67] |
|
| [68] |
|
| [69] |
|
| [70] |
|
| [71] |
|
| [72] |
|
| [73] |
|
| [74] |
|
| [75] |
|
| [76] |
|
| [77] |
|
| [78] |
|
| [79] |
|
| [80] |
|