


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
气管导管套囊内注入利多卡因预防气管插管全麻术后患者气道并发症的系统评价
[黎安良, 高鸿 , 林少锋, 刘艳秋]
, 林少锋, 刘艳秋]
, 林少锋, 刘艳秋]
|
|


系统评价通过气管导管套囊内注入利多卡因预防气管插管全麻术后患者咽喉痛、呛咳及声音嘶哑的效果。
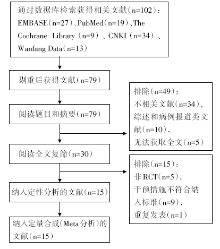
方法采用Cochrane系统评价方法,计算机检索The Cochrane Library、PubMed、EMBASE、CNKI和Wanfang Data数据库,同时手工检索图书馆馆藏期刊,收集有关套囊内注入利多卡因预防全麻患者术后咽喉痛的随机对照试验,检索时限均截止于2015年10月。由两位研究者按照纳入与排除标准筛选文献、提取资料和评价质量,然后采用RevMan 5.1软件进行Meta分析。
结果最终纳入15个随机对照试验,共982例患者。Meta分析结果显示:①咽喉痛发生情况:在术后1 h内咽痛发生人数试验组少于对照组[比值比=0.31,95%可信区间(0.17,0.57), P=0.000 2];术后24 h内咽痛发生人数试验组少于对照组[比值比=0.34,95%可信区间(0.17,0.68), P=0.002]。②术后咽痛严重程度评分:术后1 h内咽痛严重程度评分试验组低于对照组[加权均数差=-18.08,95%可信区间(-26.05,-10.11), P<0.000 01];术后24 h咽痛严重程度评分试验组低于对照组[加权均数差=-10.11,95%可信区间(-12.13,-8.08), P<0.000 01]。③术后苏醒期呛咳发生情况:试验组呛咳发生人数较少[比值比=0.26,95%可信区间(0.13,0.53), P=0.000 2]。④术后24 h声音嘶哑发生情况:试验组声音嘶哑发生人数较少[比值比=0.29,95%可信区间(0.11,0.75), P=0.01]。
结论术中通过气管导管套囊内注入利多卡因可以有效预防术后全麻气管插管患者咽喉痛、声音嘶哑及呛咳的发生。
Objective To systematically review preventive effect that intracuff Lidocaine used in patients receiving general anesthesia endotracheal intubation is associated with significantly reduced incidence of postoperative sore throat, cough and hoarseness. Methods Using the Cochrane systematic review methods, we searched the Cochrane Controlled Trial Registers (CCTR) of the Cochrane Library, PubMed, EMBASE, CNKI and Wanfang databases from inception to October 2015. We also handsearched relevant journals and conference proceedings. Two reviewers independently selected studies and assessed the quality of the trials. Disagreements were resolved by discussion, in consultation with a third reviewer. Then, meta-analysis was performed using RevMan 5.1 software. Results Thirteen trials involving 982 patients were finally included. Meta analysis results show that the number of sore throat that occurred in the postoperative 1 h in the test group were less than the control group [OR=0.31,95%CI (0.17, 0.57), P=0.000 2]; the number of test group postoperative sore throat in 24 h occurred less than the control group [OR=0.34,95%CI(0.17,0.68), P=0.002]. The severity score of postoperative sore throat in the 1 h was less in test group than in control group [WMD=-18.08,95%CI(-26.05,-10.11), P<0.000 01]; The severity score of postoperative sore throat in the 24 h was less in test group than in control group[WMD=-10.11,95%CI (-12.13, -8.08), P<0.000 01]. The incidence of cough in the recovery period was compared with control group, and the incidence of cough in the experimental group was less than control group [OR=0.26,95%CI(0.13,0.53), P=0.000 2]. In postoperative 24 h, the incidence of hoarseness in the test group occurred less [OR=0.29,95%CI(0.11,0.75), P=0.01]. Conclusion The intracuf Flidocaine can be effective in preventing postoperative sore throat, hoarseness and choking cough for general anesthesia under tracheal intubation patients.
全身麻醉气管插管后常常出现相关并发症, 如咽喉痛、声音嘶哑、吞咽困难、咳嗽等, 其中咽喉痛最为常见, 发生率可达50%以上[1, 2, 3, 4]。一直以来临床上常常通过静脉和局部应用利多卡因来减轻全麻术后出现的咽喉痛、声音嘶哑等[5, 6, 7, 8]。目前国内外有研究报道通过套囊内注入利多卡因可减轻对气管的刺激[9, 10, 11, 12], 可通过气囊的半透膜向外渗透起到诱导气管麻醉的作用, 同时有研究报道当盐酸利多卡因被碱化时, 解离出非离子型药物, 会大大增加局麻作用[13, 14]。本研究对利多卡因注入气管插管套囊内预防术后咽痛发生的随机对照试验进行系统评价, 为其临床合理应用提供更可靠的证据。
1.1.1 纳入标准研究类型为随机对照试验, 全身麻醉下气管插管的成年患者, 不分性别和种族。
1.1.2 排除标准(1)所有的病例回顾性的文献研究和有关叙述性案例列举; (2)专家经验、医家自述和评论综述类文献; (3)已搜集术前有合并症患者的研究; (4)重要数据资料不全的文献; (5)重复发表的文献。
1.1.3 干预措施试验组套囊内注入利多卡因, 对照组套囊内注入空气或生理盐水。
主要指标:①术后1小时和24小时咽喉痛的发生情况; ②术后1小时和24小时咽喉痛严重程度评分; ③术后苏醒期呛咳的发生情况; ④术后24小时声音嘶哑发生情况。
计算机检索The Cochrane Library、PubMed、MEDLINE、EMBASE、CNKI和Wanfang Data数据库; 对所获文献的参考文献进行筛查; 查阅各种会议记录, 研究生论文等。
英文检索词:(cuff OR cuffs OR intracuff)AND (lidocaine OR lignocaine OR xylocaine)AND (Sore throat OR Sore throats OR throat Sore OR pharyngalgia OR throat pain OR postoperative sore throat OR pharyngeal discomfort OR pharyngeal complication OR airway discomfort OR airway complication OR throat discomfort)。
中文检索词:套囊; 套囊内; 利多卡因; 咽痛; 咽喉痛; 咽喉疼。
由两位研究人员根据纳入和排除标准, 分别对文献进行筛选, 并交叉核对, 如遇分歧通过讨论或咨询第三方解决, 然后采用统一的资料提取表提取各纳入研究的基本资料。
采用Cochrane系统评价员手册5.1.0[15]随机对照试验的偏倚评估风险评估工具评价纳入研究的方法学质量。评价内容包括:①随机方法是否正确; ②是否实施分配方案隐藏; ③是否采用盲法; ④是否存在缺失数据所致偏倚; ⑤是否存在选择性报告所致偏倚; ⑥是否存在其他类型的偏倚。同时采用Jadad评分[16]评价文献质量, 评分标准:是否采用随机(0~2分:未叙述随机为0分, 仅叙述随机为1分, 描述正确的随机办法为2分); 是否使用盲法(0~2分:未叙述为0分, 仅叙述双盲为1分。操作者和随访者双盲为2分); 失访的原因(0~1分:未叙述为0分, 叙述为1分)。总分3分以上为高质量文献。
采用Cochrane协作网提供的RevMan 5.1软件进行统计分析。对二分类变量采用比值比(odds ratio, RR), 度量衡单位相同的连续性变量采用加权均数差(weighted mean difference, WMD), 不同则采用标准化均数差(standardized mean difference, SMD), 两者均以95%可信区间(confidence interval, CI)表示。采用2检验进行异质性分析(检验标准P=0.05), 不存在异质性(P> 0.5)时, 以固定效应模型进行Meta分析; 存在异质性(P≤ 0.5)时, 分析异质性来源, 采取分层分析或去除异质性大的研究, 再用固定效应模型进行合并分析, 若有足够临床同质性时采用随机效应模型。异质性源于低质量研究时, 则对Meta分析结果进行敏感性分析。
初检获得相关文献30篇, 通读全文, 其中15篇文献符合纳入标准[9, 12, 13, 14, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27], 国内文献1篇, 其余为国外文献, 包括共982名(试验组493名和对照组489名)患者, 文献筛选流程及结果见图1。
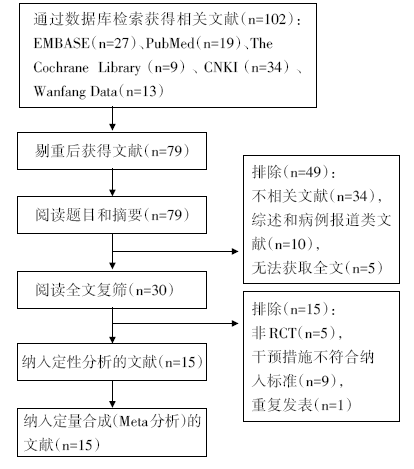 | 图1 文献筛选流程及结果 |
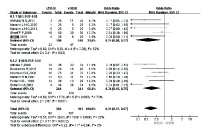
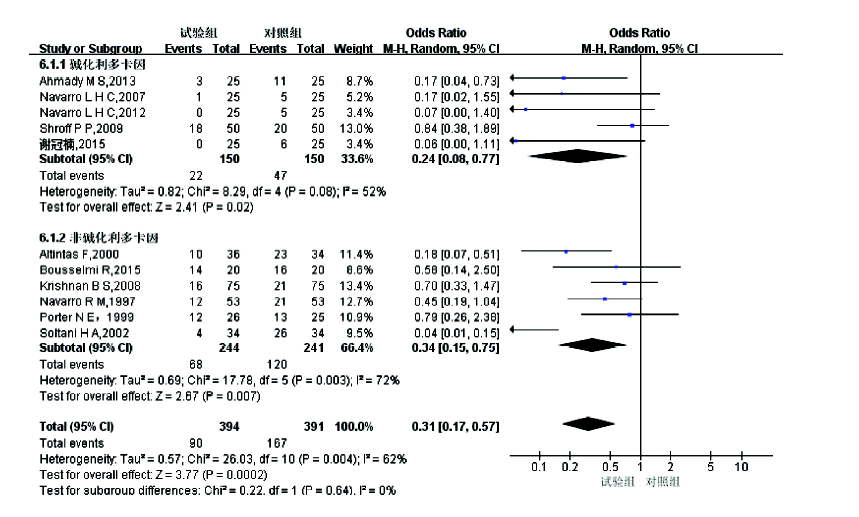
2.3.1 咽喉痛发生情况Meta分析
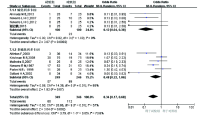
各研究结果之间存在异质性, 采用随机效应模型分析, 结果显示在术后1小时内咽痛发生人数验组少于对照组[OR=0.31, 95%CI(0.17, 0.57), P=0.000 2]; 术后24小时内咽痛发生人数试验组少于对照组[OR=0.34, 95%CI(0.17, 0.68), P=0.002]。亚组分析中, 碱化和非碱化利多卡因在术后1小时内和24小时咽痛发生人数均少于对照组, 详见图2和图3。
 | 图2 术后1小时内咽痛发生情况的Meta分析 |
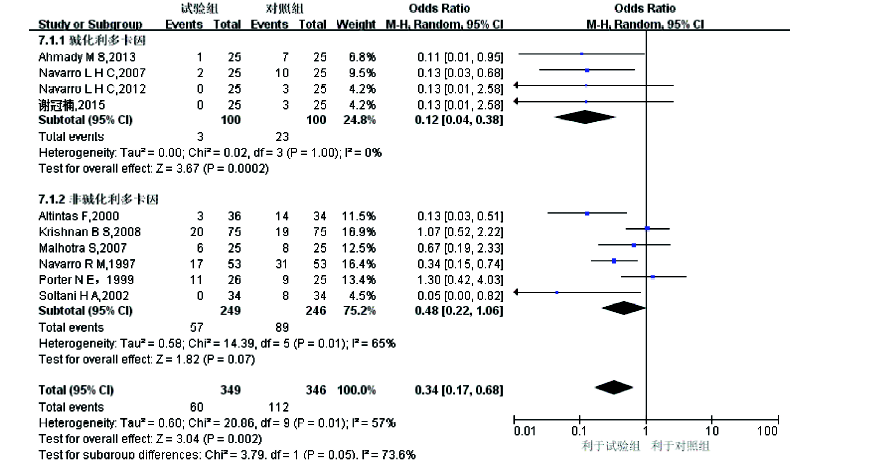 | 图3 术后24小时咽痛发生情况的Meta分析 |
2.3.2术后咽痛严重程度评分Meta分析
2.3.2.11 小时内咽痛发生情况
各研究结果之间存在异质性, 采用随机效应模型分析, 结果显示术后1小时内咽痛严重程度评分试验组低于对照组[WMD=-18.08, 95%CI(-26.05, -10.11), P< 0.000 01], 见图4。
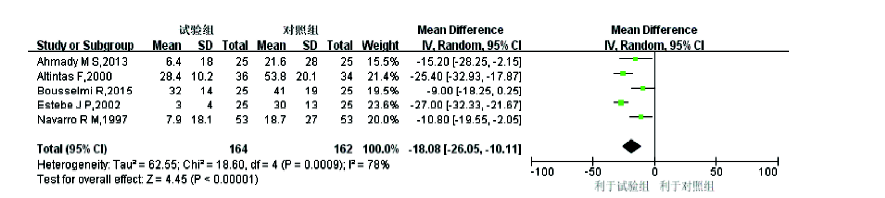 | 图4 术后1小时咽痛严重程度的Meta分析 |
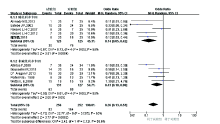
2.3.2.224小时咽痛发生情况
各研究结果之间无异质性, 采用固定效应模型分析, 术后24小时咽痛严重程度评分试验组低于对照组[WMD=-10.11, 95%CI(-12.13, -8.08), P< 0.000 01], 见图5。
 | 图5 术后24小时咽痛严重程度的Meta分析 |
2.3.3 术后苏醒期呛咳发生情况的Meta分析
各研究结果之间无异质性, 采用固定效应模型分析, 结果显示与对照组比较; 试验组呛咳发生人数较少[OR=0.26, 95%CI(0.13, 0.53), P=0.000 2], 见图6。
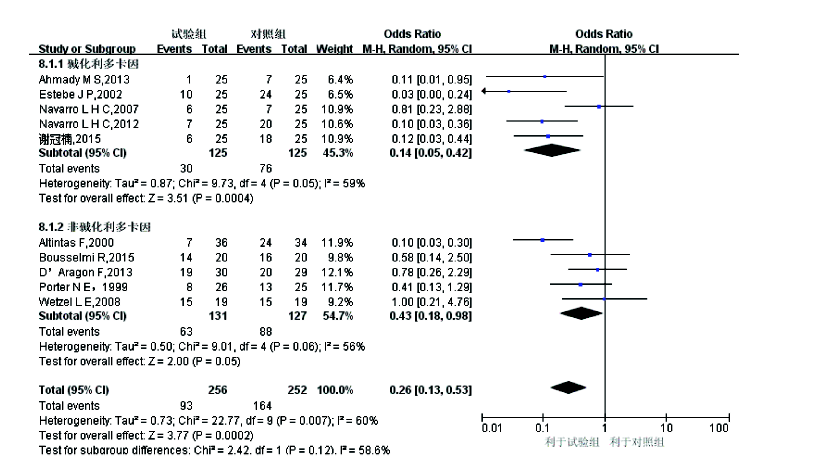 | 图6 术后苏醒期呛咳发生情况的Meta分析 |
2.3.4 术后24小时声音嘶哑发生情况的Meta分析
各研究结果之间存在异质性, 采用随机效应模型分析, 结果显示与对照组比较, 试验组声音嘶哑发生人数较少[OR=0.29, 95%CI(0.11, 0.75), P=0.01], 见图7。
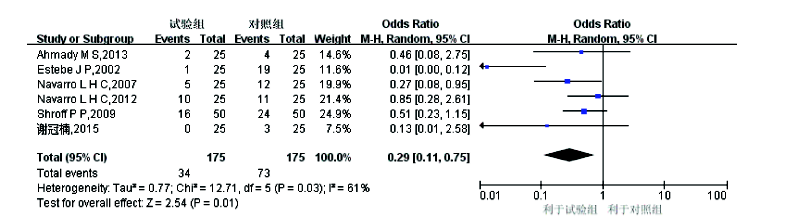 | 图7 术后24小时声音嘶哑发生情况的Meta分析 |
全身麻醉后患者抱怨咽痛、咳嗽、声音嘶哑等不适, 成为一直困扰着临床医生的问题, 其原因常常由气管插管操作过程及带管期间的机械损伤和压迫气道黏膜导致损伤、水肿。目前临床上采用许多办法试图预防术后相关并发症的发生, 如术前口腔内喷雾激素或局麻药物, 静脉预防性注射激素, 导管涂抹激素或喷洒局麻药以及非甾体抗炎药的局部应用等[8, 28, 29, 30], 但效果不尽相同, 而且由药物引起的副作用也成为医生的顾虑。近年, 一些报道在套囊内注入利多卡因可以有效降低术后并发症的发生, 本研究搜集数据库里所有相关文献统计后予分析。
本系统评价结果显示通过套囊内注入利多卡因, 可以有效减少术后咽痛、声音嘶哑的发生, 而且术后可以耐受气管插管, 患者发生呛咳少, 术后患者咽喉痛严重程度较对照组轻。由于盐酸利多卡因通过套囊渗透到气道壁黏膜起局部麻醉作用, 因此患者术后气道不适感降低。早年Sconzo等[31]通过实验发现利多卡因可以透过气管导管套囊壁, 并首次提出套囊内利多卡因技术这一概念, 即利用利多卡因填充气管导管套囊, 使其成为局麻药的缓释容器, 缓慢渗透利多卡因, 麻醉与套囊相接触的气管黏膜, 抑制咳嗽反射, 同时减轻诸如咽痛、声音嘶哑、发声困难、吞咽困难等气管插管相关并发症。随后Navarro 和 Baughman[17]首次将套囊内利多卡因技术应用于临床, 观察到术后咽痛得到了显著的改善。Matias 首次通过向利多卡因溶液中加入 NaHCO3使利多卡因对气管导管套囊的通透性升高了 63 倍, 其后相继有研究者证实碱化利多卡因在气管导管套囊内通透性高, 并通过临床试验验证了气管导管套囊内填充碱化利多卡因可在 2 小时后阻滞快适应性感受器, 可极大地抑制咳嗽反射, 使拔管更加平顺, 患者术后咽痛明显减轻, 且吞咽反射未受影响, 没有出现声带麻痹。
气管导管套囊通常由聚氯乙烯制作, 聚氯乙烯是一种高度疏水但脂溶性很高的物质。同局麻药透过硬脊膜的机制相类似, 只有非离子化的利多卡因可以透过气管导管套囊壁, 通过碱化利多卡因溶液提高其 pH 值, 为最常用的增加非离子化利多卡因的方法。本研究结果显示两个亚组碱化和非碱化利多卡因注入套囊内均可有效降低术后咽痛的发生, 并且术后咽痛严重程度较轻。
本系统评价的局限性:本研究共纳入15项研究, 存在Jadad评分小于3分的低质量文献, 且样本量较少, 可能会对结果造成偏倚。纳入研究对象中, 患者吸烟史不同, 可能存在一定异质性。各研究的干预措施在具体细节方面及测量指标的描述也不尽相同, 可能造成测量偏倚。本系统评价纳入文献语种主要为英文和中文, 排除其它语种, 可能造成分布偏倚。因此, 在套囊内注入利多卡因是否能对患者术后并发症预防有效、更安全, 尚需更多高质量、大样本随机对照研究验证。
The authors have declared that no competing interests exist.
| [1] |
|
| [2] |
|
| [3] |
|
| [4] |
|
| [5] |
|
| [6] |
|
| [7] |
|
| [8] |
|
| [9] |
|
| [10] |
|
| [11] |
|
| [12] |
|
| [13] |
|
| [14] |
|
| [15] |
|
| [16] |
|
| [17] |
|
| [18] |
|
| [19] |
|
| [20] |
|
| [21] |
|
| [22] |
|
| [23] |
|
| [24] |
|
| [25] |
|
| [26] |
|
| [27] |
|
| [28] |
|
| [29] |
|
| [30] |
|
| [31] |
|